Busan Tests Trauma Network as Hospital Acceptance Comes Into Focus
Busan’s new trauma-care pilot is less about adding hospital names than about how emergency decisions are made. The city will need to show how patients are routed, why hospitals accept or refuse them and when cases are escalated to the regional trauma center.
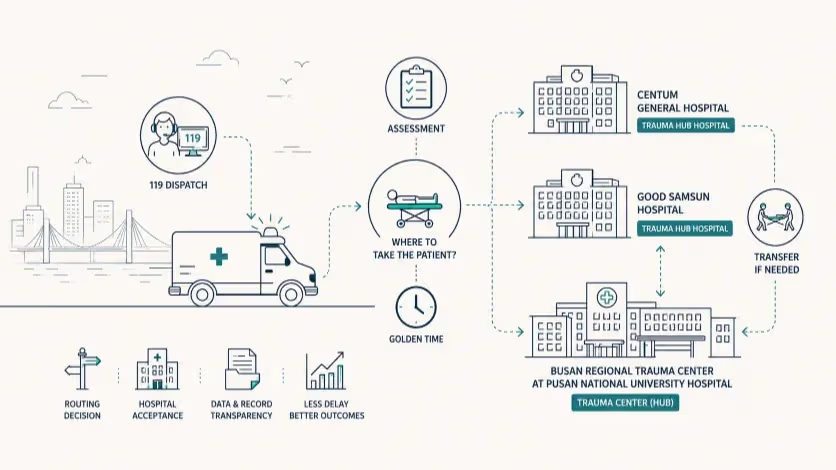
The city has assigned Centum General Hospital and Good Samsun Hospital new roles in trauma care. The program’s effect will depend on how clearly 119 crews, regional trauma hub hospitals and the Busan Regional Trauma Center divide decisions over assessment, stabilization and transfer.
Busan has begun a nine-month trauma-care pilot that gives two local hospitals a formal role in receiving and stabilizing some trauma patients before they are transferred, if necessary, to the Busan Regional Trauma Center at Pusan National University Hospital.
The city launched the program Friday at the Busan Regional Trauma Center, designating Centum General Hospital and Good Samsun Hospital as regional trauma hub hospitals under a hub-and-spoke model. Pusan National University Hospital remains the hub for complex surgery and intensive care, while the two designated hospitals are expected to handle initial assessment and stabilization. The city’s own project outline places the pilot between April and December, with 955 million won in municipal funding. Public reports on the launch also describe the same division of labor among the regional trauma center, the two designated hospitals and the Busan Fire Disaster Headquarters.
The program is being introduced in the language of “golden time,” but the phrase covers several separate decisions. A patient has to be taken somewhere. A hospital has to agree to receive the patient. Someone has to decide whether the case can be handled at the first hospital or needs the Busan Regional Trauma Center. If the first hospital cannot provide definitive care, transfer has to be arranged before the initial stop becomes a delay.
The city has named the institutions. It has not yet publicly shown enough of the operating rules to know how those decisions will be made in the field. For a 119 crew, the practical question will be whether a patient should be taken to Centum General Hospital, Good Samsun Hospital or directly to the Busan Regional Trauma Center. For the two regional trauma hub hospitals, it will be whether they are expected to accept certain trauma categories unless a defined exclusion applies. For the regional trauma center, it will be how early it is brought into a case that may need escalation.
The designation is therefore only the first layer of the policy. The harder part is the sorting rule behind it: which patients are appropriate for a spoke hospital, which patients should bypass the spokes, and which patients should be transferred after the first assessment.
Why distance alone is not enough
Trauma care does not fit neatly into the ordinary assumption that the nearest emergency room is the safest destination. A nearby hospital may be able to receive a patient quickly but still lack the surgeon, CT access, blood supply, operating room, anesthesia coverage or intensive-care bed needed for a patient with internal bleeding, severe head injury or multiple injuries. A more advanced trauma center may be better equipped but farther away, or already under pressure from other critical patients.
Field triage guidelines used in mature trauma systems treat the destination as a clinical decision. The American College of Surgeons says the national field triage guidelines used in the United States are intended to support EMS clinicians in transport-destination decisions so that seriously injured patients reach the most clinically appropriate trauma centers. That principle is directly relevant to Busan’s pilot because the policy does not merely add hospital names to a list; it asks 119 crews to sort patients between local stabilization and regional trauma-center care.
The trade-off is familiar in trauma systems. If a seriously injured patient is taken first to a hospital that cannot provide definitive treatment, the patient may lose time to a second transfer. If too many patients are sent directly to the highest-level center, the hub can become crowded with cases that might have been assessed or stabilized elsewhere. Busan’s model tries to place two regional trauma hub hospitals between those outcomes.
The difficulty is that the difference between those patients is not always visible at the scene. A fall, traffic crash or workplace injury may produce a patient who appears stable before imaging. A head injury can become more serious after the first assessment. A fracture can accompany internal injury. A patient who initially looks suitable for local stabilization may need surgery, neurosurgical review, blood transfusion or ICU care sooner than expected.
That is where the pilot can add time as well as save it. If the spoke hospital has the right staff and resources available, the first stop can produce faster assessment and a better transfer decision. If the hospital has to search for imaging, a specialist, an ICU bed or a receiving team at the Busan Regional Trauma Center, the first stop becomes one more stage in the patient’s route.
The numbers behind the policy
The case for improving trauma coordination is strong at the national level. South Korea’s preventable trauma death rate fell from 30.5 percent in 2015 to 9.1 percent in 2023, according to the Ministry of Health and Welfare. The ministry defines the rate as the share of trauma deaths judged likely to have been avoidable if appropriate care had been provided in time, and it links the long-term decline to policy efforts including the expansion and operation of regional trauma centers.
The Busan-related picture is more complicated. The Busan-Daegu-Ulsan-Gyeongsang region recorded a 2023 preventable trauma death rate of 11.4 percent, higher than the national figure. The region improved from 13.5 percent in 2021, but the drop was 2.1 percentage points, smaller than the declines recorded in several other regions. The same ministry release notes that Busan’s data submission rate for the national trauma death review was 60.9 percent and that low submission rates may lead to underestimation of preventable deaths.
That caveat changes the way the pilot should be read. The issue is not only whether Busan can move patients faster. It is whether the city can produce a cleaner record of what happened between injury and treatment: where a patient was first taken, how many hospitals were contacted, why a hospital declined, when imaging occurred, when transfer was ordered and whether the Busan Regional Trauma Center was involved before the case deteriorated.
The Korea Disease Control and Prevention Agency’s 2024 severe-injury data also point to the need for more precise local analysis. Busan recorded 398 severe trauma cases by accident location in 2024, down from 440 in 2023. The city’s median time from emergency call to hospital arrival for severe trauma cases was 34 minutes in 2024, close to the national median of 35 minutes but longer than Busan’s 28 minutes in 2016. The same dataset shows that severe trauma cases nationwide remain in the 8,000 range annually, with 8,170 cases in 2024.
A longer transport time is not automatically a sign of failure. It can reflect traffic, geography, on-scene treatment, the time needed to assess a patient, or a deliberate choice to bypass a nearer hospital for a more appropriate one. But those explanations require data that separate delay from clinical routing. If a 34-minute median reflects better matching to suitable hospitals, the policy reading is different from a 34-minute median caused by repeated calls to hospitals that cannot accept the patient.
The missing detail is the operating rule
Busan’s announcement emphasizes cooperation among the city, the fire authorities, the regional trauma center and the two participating hospitals. Cooperation matters, but trauma routing depends on rules that can be used at night, during weekends, and when a patient’s condition is changing.
The central government’s emergency-transport pilot offers a useful comparison. In February, the Ministry of Health and Welfare and the National Fire Agency announced a separate emergency patient transport innovation pilot in Gwangju, North Jeolla and South Jeolla. That project calls for region-specific transport guidelines, stronger sharing of patient and hospital resource information, support from regional emergency medical situation rooms for serious emergency patients, and designation of priority acceptance hospitals when hospital selection is delayed. It also refers to real-time information on resources such as ICU beds, operating rooms, CT and MRI capacity.
That national design raises a concrete question for Busan’s trauma project. Are Centum General Hospital and Good Samsun Hospital simply designated partners, or will they operate under patient categories and acceptance rules clear enough for 119 crews to rely on? If a hospital declines a patient, will the reason be logged as lack of ICU capacity, no specialist coverage, operating-room limits, emergency-room saturation, direct-to-hub severity or another defined category? If a spoke hospital accepts a patient and then needs to transfer, does the Busan Regional Trauma Center become involved at the first sign of severity, after imaging, or only after the local hospital asks for transfer?
The answers matter because “hospital refusal” can describe very different events. A hospital that declines because the patient should go directly to the Busan Regional Trauma Center is making a different decision from a hospital that declines because it lacks a surgeon, has no ICU bed or has a saturated emergency department. A useful pilot would separate those cases rather than count them under one label.
That distinction is also important for deciding what Busan should do next. If refusals cluster around ICU shortages, the city is looking at bed capacity. If they cluster around specialist absence, the issue is coverage. If the two regional trauma hub hospitals rarely receive trauma patients from 119 crews, the problem may be dispatch confidence or unclear routing. If they receive patients but transfer many of them after long stays, the question shifts to transfer triggers and early hub consultation.
Readiness by hour, not by title
Centum General Hospital and Good Samsun Hospital now have a more specific role than ordinary emergency departments in this pilot. They are being asked to serve as the first clinical decision point for some trauma patients, which means their capacity has to be understood by time of day and by injury type.
A hospital may be able to assess and stabilize a trauma patient on a weekday afternoon but face a different situation at 2 a.m. on a Sunday if imaging is busy, the surgeon is on call from outside the hospital, anesthesia coverage is limited or the ICU is full. A formal designation does not answer those questions. The pilot data should.
The list of practical resources is not exotic. A regional trauma hub hospital needs rapid triage, emergency physicians, nurses trained for trauma cases, CT access, blood availability, surgical consultation, anesthesia support, an operating-room plan, ICU access and a direct line to the Busan Regional Trauma Center. The issue is not whether each resource exists somewhere in the hospital, but how quickly it can be activated when a patient arrives.
Pusan National University Hospital faces a related burden. If the two regional trauma hub hospitals take the right patients and transfer early when needed, the Busan Regional Trauma Center may receive more appropriate cases with better warning. If the spokes delay transfer or if the hub is already constrained by ICU occupancy, operating-room access or specialist workload, the network can slow down at the point where it is supposed to concentrate expertise.
That makes the pilot less a test of whether two hospitals can participate and more a way to locate the actual bottleneck. Delay before acceptance points toward dispatch coordination and hospital-selection rules. Delay after arrival at a regional trauma hub hospital points toward imaging, specialist response or local capacity. Delay during transfer points toward hub availability, ambulance support or escalation authority.
Each pattern would call for a different policy response. Treating the pilot as one overall success or failure would miss the point.
What the December data should show
By December, Busan is unlikely to have enough cases to make a clean claim about preventable trauma deaths. Severe trauma cases are varied, and the pilot period is short. A useful evaluation should start with the operational record.
For each case handled through the pilot, the city should be able to reconstruct the route: the injury location, the first destination, the reason for that destination, the number of hospital contacts before acceptance, the time to confirmed acceptance, whether a designated regional trauma hub hospital declined, the recorded reason for any refusal, and the time from arrival to CT, transfusion, surgery, ICU admission or transfer decision when those steps apply.
Transfer cases need their own analysis. If a patient moves from Centum General Hospital or Good Samsun Hospital to Pusan National University Hospital, the record should show whether the transfer was expected from the beginning, triggered by imaging, caused by deterioration or forced by a resource gap at the first hospital. The policy response would differ in each case. A high rate of expected transfers may mean the spokes are functioning as rapid assessment points. A high rate of delayed transfers after long stays would suggest that the threshold for escalation is too late.
Aggregate disclosure would be enough for public accountability. Busan does not need to publish private patient information, but it could release monthly trauma volumes, median transport times, acceptance rates, average hospital contacts, refusal reasons, transfer times and the share of patients routed through each part of the network. Those figures would show whether the system is changing in the parts of the route where delay usually hides.
The most useful outcome this year may be a map of delay rather than a mortality claim. If 119 crews do not use the two regional trauma hub hospitals often, Busan will need to look at routing criteria and confidence in the spoke hospitals. If the hospitals accept patients but transfer many after delays, the city will need to examine specialist availability, ICU capacity and transfer triggers. If the Busan Regional Trauma Center still receives most severe cases without early notice from the spokes, the issue will be coordination rather than geography.
That is a narrower conclusion than the language of “golden time,” but it is more useful. The pilot will matter if it shows where the emergency route slows down and which institution has the power to shorten that part of the route.
Editorial Context
"Independent journalism relies on radical transparency. View our full log of editorial notes, corrections, and project dispatches in the Newsroom Transparency Log."
Reader Pulse
The report's impact signal
Be the first to provide a reading pulse. These collective signals help our newsroom understand the impact of our reporting.
Join the discussion
A more thoughtful conversation, anchored to the story
Atlantic-style discussion for this article. One-level replies, editor prompts, and moderation-first participation are now powered directly by Prisma.
Discussion Status
Open
Please sign in to join the discussion.
The Weekly Breeze
Independent reporting and analysis on Busan,
Korea, and the broader regional economy.






